Official Cna Shower Sheets Form in PDF
Official Cna Shower Sheets Form in PDF
The CNA Shower Sheets form serves as a vital tool in the monitoring of residents' skin health during their bathing routines. This form is designed to guide Certified Nursing Assistants (CNAs) in conducting a thorough visual assessment of a resident’s skin while providing showers. It emphasizes the importance of identifying and documenting any abnormalities, such as bruising, skin tears, rashes, and other skin conditions. The form includes a body chart that allows CNAs to accurately mark the location of any issues, ensuring that each abnormality is clearly described and communicated. In addition to the visual assessment, the form prompts CNAs to consider whether the resident requires toenail care, further contributing to the overall well-being of the individual. After the initial assessment, the CNA is responsible for reporting any findings to the charge nurse, who will then evaluate the situation and determine the necessary interventions. This process promotes a collaborative approach to resident care, as any concerns can be forwarded to the Director of Nursing (DON) for additional review. By utilizing this form, CNAs play a crucial role in maintaining skin integrity and addressing potential health issues promptly.
Hiv Negative Results Letter - Important record for data collection and monitoring.
Who Can Write an Esa Letter - The right ESA letter can provide peace of mind and the comfort of having your furry friend by your side.
Mortgage Interest Tax Form - Important messages regarding partial payments explain how they are handled by your servicer.
Filling out the CNA Shower Sheets form is an essential task that ensures accurate documentation of a resident’s skin condition during showers. Properly completing this form helps maintain the health and safety of residents by allowing for timely reporting and intervention when necessary.
When filling out and using the CNA Shower Sheets form, consider the following key takeaways:
Misconceptions about the CNA Shower Sheets form can lead to confusion and mismanagement of resident care. Here are six common misunderstandings:
Understanding these misconceptions can help ensure that residents receive the best possible care. Proper use of the CNA Shower Sheets form is vital for effective communication and monitoring.
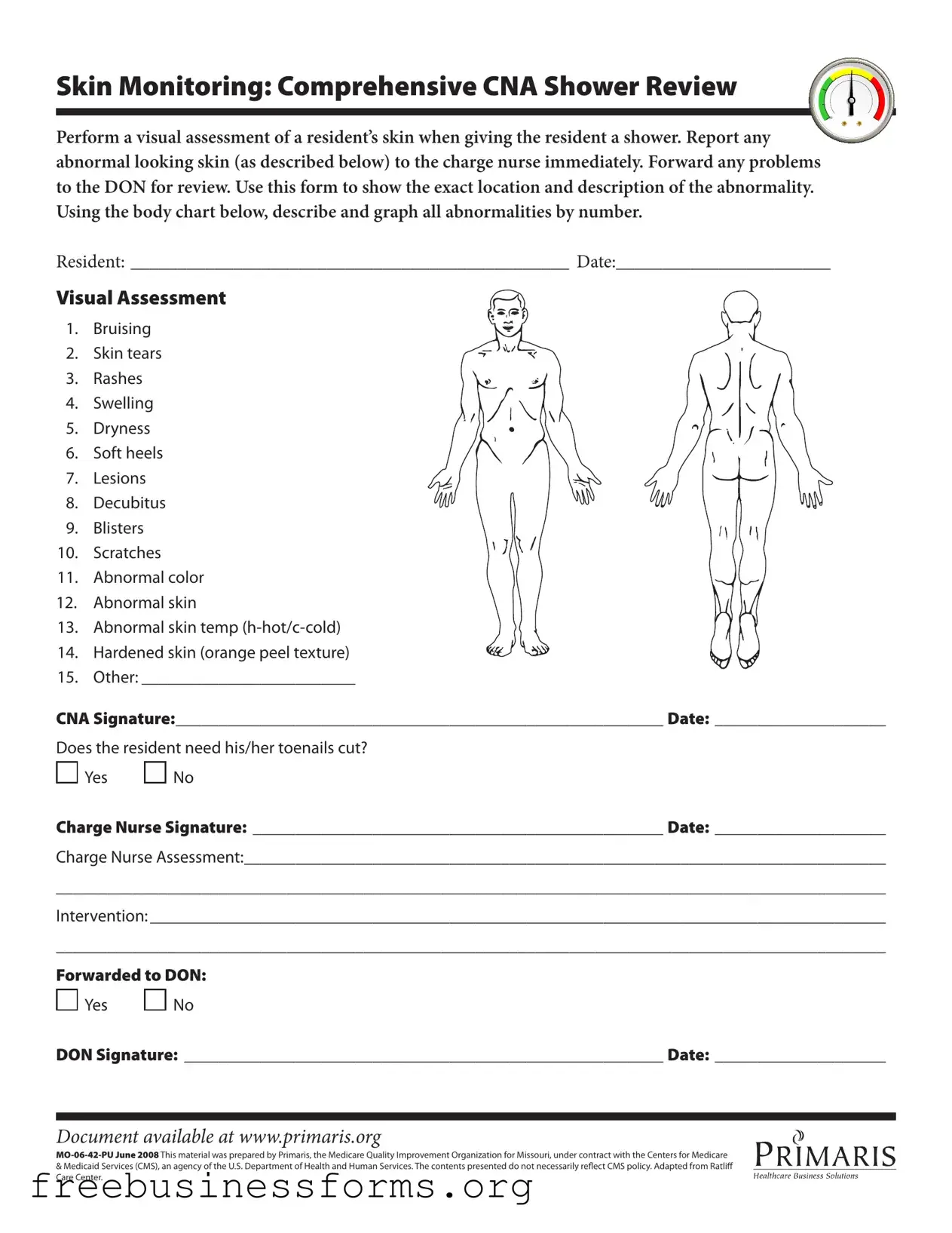
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
| Fact Name | Fact Description |
|---|---|
| Purpose | The CNA Shower Sheets form is designed for documenting skin assessments during resident showers. |
| Skin Monitoring | The form emphasizes the importance of visual assessments for identifying abnormalities in residents' skin. |
| Immediate Reporting | Any abnormal skin findings must be reported to the charge nurse without delay. |
| Documentation | The form includes a body chart for graphically representing the location of skin abnormalities. |
| Assessment Categories | Categories for assessment include bruising, skin tears, rashes, and more, totaling fifteen distinct observations. |
| Toenail Care | The form inquires whether the resident requires toenail trimming, which is crucial for overall foot health. |
| Signatures Required | The form requires signatures from both the CNA and the charge nurse to validate the assessment. |
| Forwarding Protocol | Any issues noted must be forwarded to the Director of Nursing (DON) for further review. |
| Regulatory Compliance | This form is aligned with guidelines from the Centers for Medicare & Medicaid Services (CMS). |
| Document Availability | The CNA Shower Sheets form can be accessed online at www.primaris.org. |